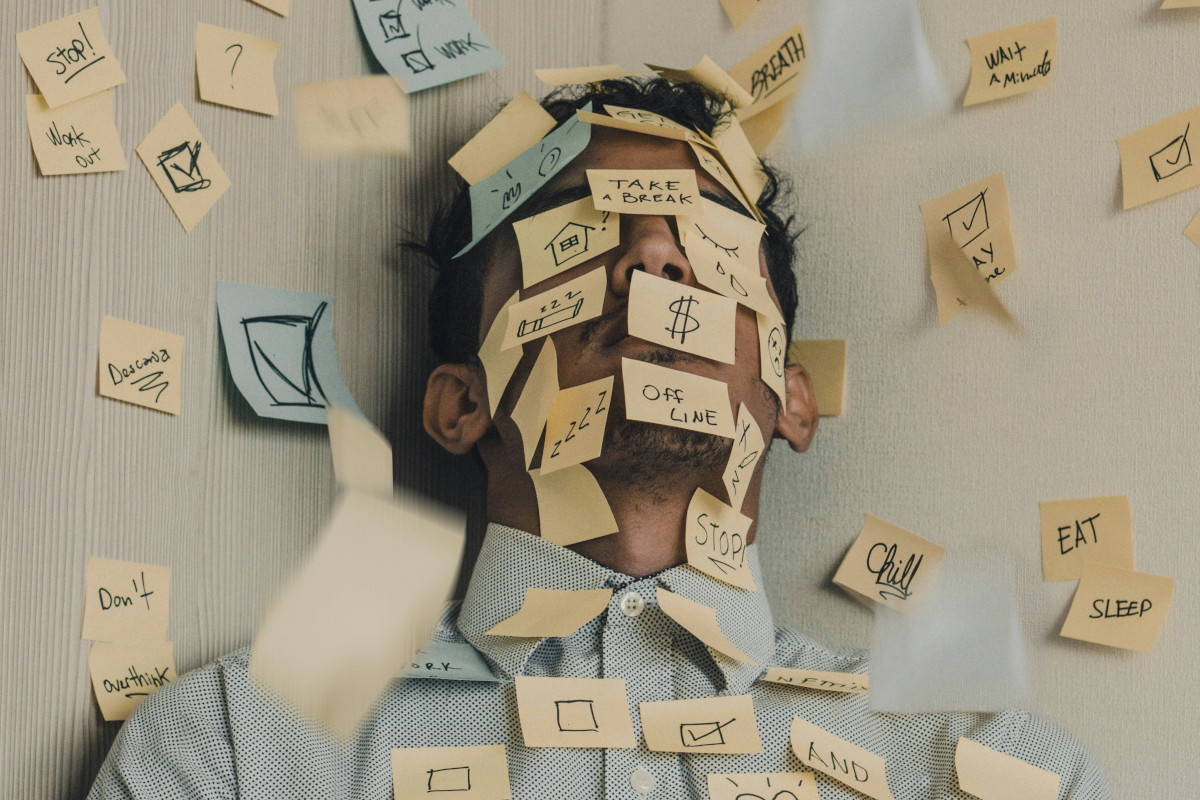
What causes tension headaches?
The kind of headache most people are familiar with – without knowing its name – is “tension-type” headache (known as “TTH” for short in the scientific community), or just “tension headache”. Tension headaches are the most widespread type of headache – but because they’re so common, they’re easily dismissed as something you can’t prevent. And yet, the very fact that tension headaches are so widespread means they should be taken seriously.
-
References
Ashina S, Mitsikostas DD, Lee MJ, Yamani N, Wang SJ, Messina R, Ashina H, Buse DC, Pozo-Rosich P, Jensen RH, Diener HC, Lipton RB. Tension-type headache. Nat Rev Dis Primers. 2021 Mar 25;7(1):24. doi: 10.1038/s41572-021-00257-2. PMID: 33767185.
Bhoi SK, Jha M, Chowdhury D. Advances in the Understanding of Pathophysiology of TTH and its Management. Neurol India. 2021 Mar-Apr;69(Supplement):S116-S123. doi: 10.4103/0028-3886.315986. PMID: 34003157.
Fu GJ, Wang LD, Chi XS, Liang X, Wei JJ, Huang ZH, Shen W, Zhang YL. Research Progress on the Experimental Model and Underlying Mechanistic Studies of Tension-Type Headaches. Curr Pain Headache Rep. 2024 May;28(5):439-451. doi: 10.1007/s11916-024-01238-2. Epub 2024 Mar 19. PMID: 38502437; PMCID: PMC11126509.
Parsaei M, Taebi M, Arvin A, Moghaddam HS. Brain structural and functional abnormalities in patients with tension-type headache: A systematic review of magnetic resonance imaging studies. J Neurosci Res. 2024 Jan;102(1):e25294. doi: 10.1002/jnr.25294. PMID: 38284839.
Pinquart, Martin & Sörensen, Silvia. (2006). Gender Differences in Caregiver Stressors, Social Resources, and Health: An Updated Meta-Analysis. The journals of gerontology. Series B, Psychological sciences and social sciences. 61. P33-45. 10.1093/geronb/61.1.P33.
Qin L, Song P, Li X, Yang L, Xu F, Zhu X, Cai L, Hu G, Sun W, Zhang Y, Zhang L. Tension-Type Headache Management: A Systematic Review and Network Meta-analysis of Complementary and Alternative Medicine. Pain Ther. 2024 Aug;13(4):691-717. doi: 10.1007/s40122-024-00600-x. Epub 2024 May 15. PMID: 38748200; PMCID: PMC11254882.
Repiso-Guardeño Á, Moreno-Morales N, Labajos-Manzanares MT, Rodríguez-Martínez MC, Armenta-Peinado JA. Does Tension Headache Have a Central or Peripheral Origin? Current State of Affairs. Curr Pain Headache Rep. 2023 Nov;27(11):801-810. doi: 10.1007/s11916-023-01179-2. Epub 2023 Oct 27. PMID: 37889466; PMCID: PMC10713699.
Steel SJ, Robertson CE, Whealy MA. Current Understanding of the Pathophysiology and Approach to Tension-Type Headache. Curr Neurol Neurosci Rep. 2021 Oct 2;21(10):56. doi: 10.1007/s11910-021-01138-7. PMID: 34599406.
Zhou J, Cheng S, Yang H, Lan L, Chen Y, Xu G, Yin Z, Li Z, Liu M. The brain structure and function alterations in tension-type headache: A protocol for systematic review and meta analysis. Medicine (Baltimore). 2020 Jun 12;99(24):e20411. doi: 10.1097/MD.0000000000020411. PMID: 32541463; PMCID: PMC7302660.