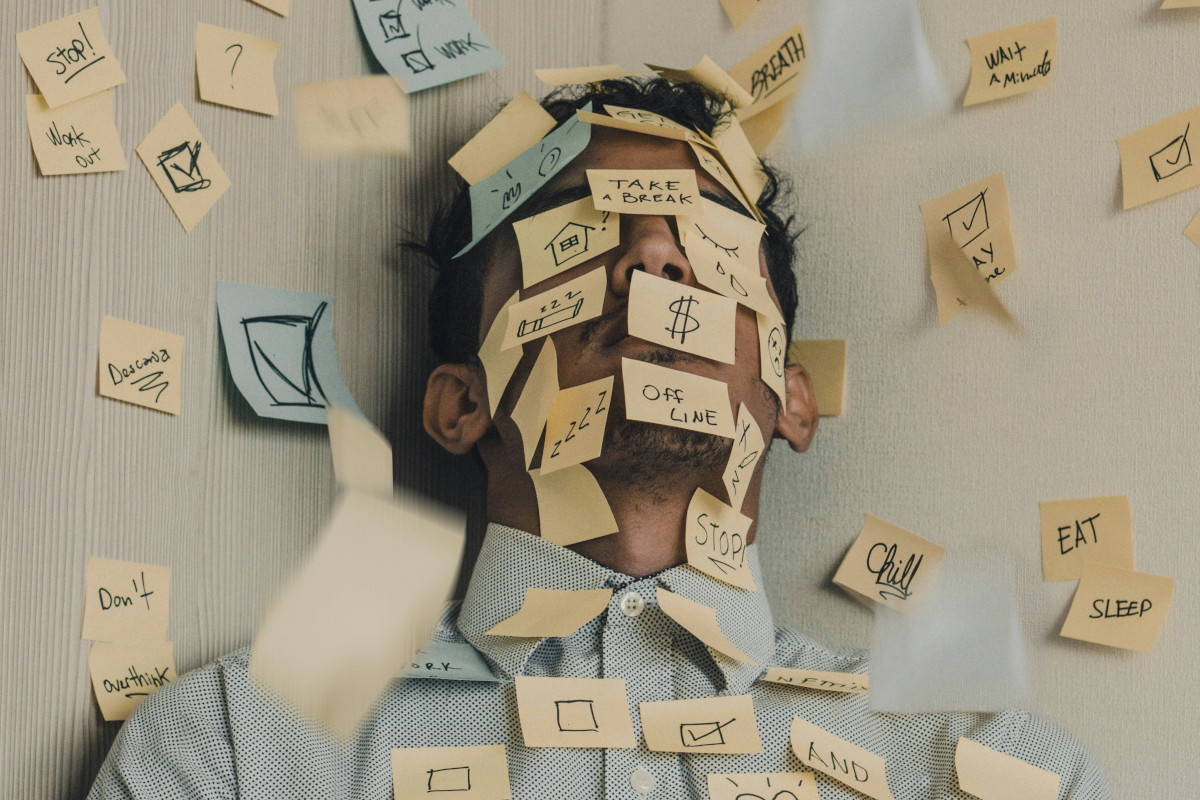
“When will the next attack come?” Living in fear of future migraine attacks
For people with migraines, the suffering often goes beyond the actual headache. As soon as the pain fades, they start worrying when the next attack is going to hit. This anxiety can have serious consequences. In fact, it can even increase the risk of new attacks and may contribute to other health issues.
-
References
Breslau N, Davis GC, Andreski P. Migraine, psychiatric disorders, and suicide attempts: an epidemiologic study of young adults. Psychiatry Res. 1991 Apr;37(1):11-23. doi: 10.1016/0165-1781(91)90102-u. PMID: 1862159.
Estave PM, Margol C, Beeghly S, Anderson R, Shakir M, Coffield A, Byrnes J, O'Connell N, Seng E, Gardiner P, Wells RE. Mechanisms of mindfulness in patients with migraine: Results of a qualitative study. Headache. 2023 Mar;63(3):390-409. doi: 10.1111/head.14481. Epub 2023 Feb 28. PMID: 36853655; PMCID: PMC10088163.
Fox J, Gaul C, Ohse J, Peperkorn N, Krutzki J, Shiban Y. Psychological transdiagnostic factors and migraine characteristics as predictors of migraine-related disability. J Headache Pain. 2025 Jul 23;26(1):167. doi: 10.1186/s10194-025-02101-4. PMID: 40702422; PMCID: PMC12285010.
Giannini G, Zanigni S, Grimaldi D, Melotti R, Pierangeli G, Cortelli P, Cevoli S. Cephalalgiaphobia as a feature of high-frequency migraine: a pilot study. J Headache Pain. 2013 Jun 10;14(1):49. doi: 10.1186/1129-2377-14-49. PMID: 23759110; PMCID: PMC3686604.
Grazzi L, Andrasik F, D'Amico D, Usai S, Rigamonti A, Leone M, Bussone G. Treatment of chronic daily headache with medication overuse. Neurol Sci. 2003 May;24 Suppl 2:S125-7. doi: 10.1007/s100720300059. PMID: 12811610.
Karimi L, Wijeratne T, Crewther SG, Evans AE, Ebaid D, Khalil H. The Migraine-Anxiety Comorbidity Among Migraineurs: A Systematic Review. Front Neurol. 2021 Jan 18;11:613372. doi: 10.3389/fneur.2020.613372. PMID: 33536997; PMCID: PMC7848023.
Kaske E, Pradela J, Otto M, John L, Derner N, Luedtke K. Factors affecting fear of attacks in patients with episodic migraine – a cross-sectional study. Cephalalgia Reports. 2025;8. doi:10.1177/25158163251345140.
Ossipova VV, Kolosova OA, Vein AM. Migraine associated with panic attacks. Cephalalgia. 1999 Oct;19(8):728-31. doi: 10.1046/j.1468-2982.1999.019008728.x. PMID: 10570728.
Raudenská J, Macko T, Vodičková Š, Buse DC, Javůrková A. Anxiety Disorders, Anxious Symptomology and Related Behaviors Associated With Migraine: A Narrative Review of Prevalence and Impact. Curr Pain Headache Rep. 2025 Jan 29;29(1):40. doi: 10.1007/s11916-024-01312-9. PMID: 39878907; PMCID: PMC11779792.
Smitherman TA, Kolivas ED, Bailey JR. Panic disorder and migraine: comorbidity, mechanisms, and clinical implications. Headache. 2013 Jan;53(1):23-45. doi: 10.1111/head.12004. Epub 2012 Dec 26. PMID: 23278473.
Stewart WF, Linet MS, Celentano DD. Migraine headaches and panic attacks. Psychosom Med. 1989 Sep-Oct;51(5):559-69. doi: 10.1097/00006842-198909000-00007. PMID: 2798702.
Suzuki K, Suzuki S, Haruyama Y, Funakoshi K, Fujita H, Sakuramoto H, Hamaguchi M, Kobashi G, Hirata K. Associations between the burdens of comorbid sleep problems, central sensitization, and headache-related disability in patients with migraine. Front Neurol. 2024 Feb 26;15:1373574. doi: 10.3389/fneur.2024.1373574. PMID: 38601337; PMCID: PMC11006273.
Takeshima T, Nakayama T, Sano H, Koga N, Matsukawa M. Association of Migraine Comorbidities with Quality of Life, Work Productivity and Daily Activities: Survey and Medical Claims Data in Japan. Adv Ther. 2025 Aug;42(8):3839-3860. doi: 10.1007/s12325-025-03236-1. Epub 2025 Jun 11. PMID: 40498280; PMCID: PMC12313757.
Yum J, Chu MK. Unraveling the connections between migraine and psychiatric comorbidities: A narrative review. Brain Dev. 2025 Aug;47(4):104392. doi: 10.1016/j.braindev.2025.104392. Epub 2025 Jul 8. PMID: 40633196.